The University of Arizona is developing “smart bandages” to detect infections after surgeries — technology that could also help Southern Arizona’s high rates of diabetes patients.
It’s part of a UA strategic priority to have artificial intelligence intersect with health-care research, which university researchers say is already transforming care.
The UA has more than $100 million in active AI-powered health-care grants, including machine-learning and LLM (Large Language Model)-enabled research, said David Ebert, the university’s chief AI and data science officer.
Machine learning is a subset of artificial intelligence that focuses on building systems that learn and improve from data, and LLM is a type of artificial intelligence trained on massive amounts of text to understand and generate human-like language.
People are also reading…
Ideas behind initiatives combining artificial intelligence and health care occurred before he got to the UA in April last year, Ebert said.

David Ebert, the University of Arizona's chief AI and data science officer.
He said he’d worked previously with Tomás Díaz de la Rubia, who is now the UA's senior vice president for research and partnerships, on matters related to AI, data science and health. He came on board as Díaz de la Rubia and UA President Suresh Garimella discussed innovation possibilities in these realms and decided to make it one of the university’s strategic priorities.
“The idea of going and getting funds from ABOR (the Arizona Board of Regents) was to accelerate and coalesce all the incredible work that’s going on — the excellence in AI, the advancement of technology, and the incredible work in the health-care space here on campus,” Ebert told the Arizona Daily Star in an interview.
Smart bandages
Geoffrey Gurtner, chair of the UA surgery department, said the idea for smart bandages arose after UA researchers identified a gap in patient treatment during surgery procedures. The goal was to monitor patients having surgeries or in the midst of direct care, during the time they go home between procedures and treatments.
In “most surgical procedures, infection is a dreaded complication,” Gurtner noted.
Also, he said, for patients who have diabetes and may have wounds on their feet, a lot of bad things can happen between the time they leave the hospital and come back in for their next treatment or checkup. They can end up needing hospital admission and amputation.
People with diabetes are at a higher risk of wound infection, and diabetes complications can include nerve damage and poor blood flow, the Mayo Clinic notes on its website. Nerve damage can keep people with diabetes from feeling skin sores or ulcers, and less blood flow can make it harder for sores to heal, Mayo says. When an ulcer causes great tissue loss or an infection that threatens a patient's life, amputation may be needed.
About 11% of the adult population in Arizona has diagnosed diabetes, while 34.5% of the adult population has prediabetes, according to the American Diabetes Association.
Specific populations in Southern Arizona, particularly the Pima (Akimel O'odham) and Tohono O'odham nations, have among the highest documented rates of type 2 diabetes in the world, with more than 50% of adults affected, the National Institutes of Health says.
So the goal of being able to diagnose deterioration and infection without a nurse or a doctor doing it provided UA's initial impetus, Gurtner said.

Lule Latifi, a research specialist at the University of Arizona's smart bandages lab, prepares experiments. The bandages have sensors that detect infection, which can be a game changer for treatment of post-surgical and diabetes patients, UA researchers say.
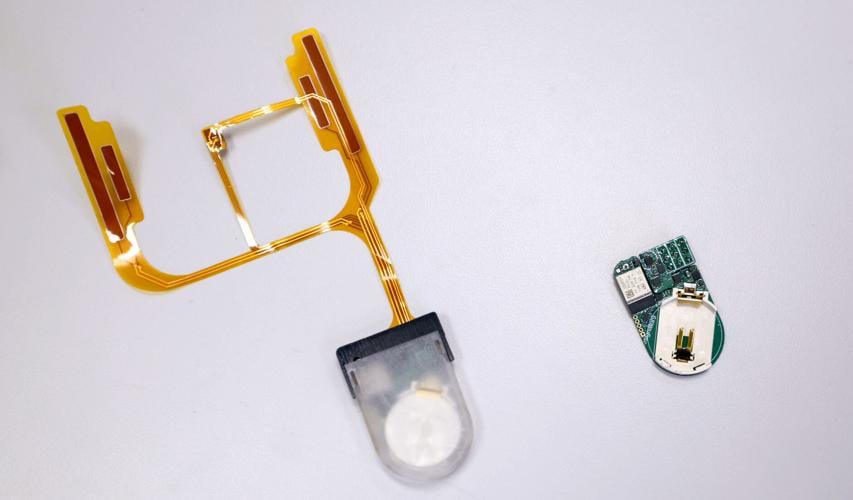
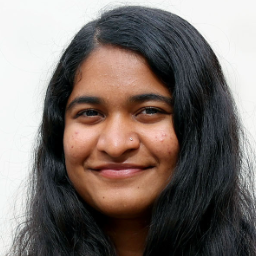
The smart bandages have “sensors that look at impedance, temperature, pH, and those indicate infection.”
Humans can spot an infection if it’s getting red, but “this is using sensors to allow a machine to make the diagnosis of infection, because you don’t have a doctor looking at your incision 168 hours a week,” he explained.
Medical practitioners will administer the smart bandages on patients before they go home after their treatments.
It’s not a problem if the bandages come in contact with water.
Gurtner said the U.S. Department of Defense would also be interested in technologies like this for future conflicts, where it might not be feasible to evacuate injured soldiers for five to seven days from austere conditions.
Such scenarios led UA researchers to think about remote monitoring of patients and autonomous treatment in low-resource conditions, he said.
He noted similar products exist in the medical market today, but said Apple watches, for instance — which offer a range of health and medical monitoring tools from passive background tracking to active diagnostic tests such as detecting heart rate — cannot diagnose infections like the smart bandages. If you have a knee replacement surgery, the Apple watch is nowhere near the knee, and it’d still require a “tremendous leap of science that is yet undiscovered” to have a watch detect infections in the knees, he said.
He said the bandages are just now being administered on patients, but the pre-clinical work of experimenting with their usage on mice, for instance, started three to four years ago. Ultimately, he said, UA’s goal would be to see the devices used on “every patient in the world” after a surgical incision to monitor non-healing wounds.

Dr. Geoffrey Gurtner, chair of the UA surgery department, explains how smart bandages work. The university is developing the technology.
The clinical trial for the bandages will be conducted at the UA, having patients wear them between doctor’s visits and collect “terabytes of data” from the devices, he said.
“When the patient comes into the office, we’re using those handheld devices and we’re gathering all that data and then we’re correlating it with what happens to the patient — do they need an amputation? Do they get septic? Do they die?” Gurtner said.
“What we found is that even with just a moment in time using those sensors, you can predict who’s going to do poorly,” he said. ”If you had 168 hours of data — all of our theories of AI and big data and machine learning suggest that the more data you have, the better your predictive value is. But even with just one moment in time, we actually can predict who’s going to end up having an infection before a doctor predicts it.”

Smart bandages being developed at the UA. The plan is to have the devices go home with patients to detect infections after surgeries — technology that could also help Southern Arizona’s high rates of diabetes patients.
AI and health-care projects
Ebert said the UA would like to use funding from the Arizona Board of Regents, which oversees the state's three public universities, to create an AI-health innovation nexus to be a facilitator and central point to link artificial intelligence and health care across campus and accelerate the research.
A few of its goals include improving discovery, research and translation, having AI-powered precision medicine, increasing access to care and improving quality of care across the state, including for Arizona’s rural population.
“It’s a key goal of ours to make sure that whether you’re located a block away from Banner UA research hospital (in Tucson) or you’re on the outskirts of Yuma, you have the same access to care and the same ability to see people,” Ebert said. “And we’re doing that through innovations and sensing technology (such as) smart wearables, telemedicine and innovations that we’re doing where we’re even able to start dialogues with patients remotely and determine what’s going on for monitoring and quality of care so that there aren’t these impediments.”
Cancer research is a priority at the UA, and the school is focusing on its cancer center for the 49th year, Ebert noted, adding that cardiovascular and neurovascular research are also areas in which the UA excels.
Additionally, the UA has expertise in research on precision aging, neurogenerative diseases, immunotherapies and cancer, Ebert said. Another focus is on “solving the challenges in rural health.”
Ebert also highlighted UA’s Arizona Simulation Technology and Education Center, which offers simulation-based training for medicine, health sciences, nursing and more. He said Arizona has been a leader in these simulations, which are now AI-powered, and it’s one way to train people faster, more effectively and give them realistic experiences.
He said the university is coming up with a timeline for specific goals, including increasing the rate of machine learning and LLM-enabled research by 10% every year in terms of publications and external funding. For external funding, the UA is looking at foundations and partnerships with federal agencies, including the Department of Defense and Energy, the National Science Foundation and the National Institutes of Health.
Integrating AI at UA’s medical schools
At UA’s colleges of medicine in Tucson and Phoenix, as well as its newly opened medical school branch in Yuma in partnership with Onvida Health, AI use is being integrated into medical education and practice, Ebert said.
He said these colleges are aware of which areas AI can be trusted in, like summarizing a prognosis, and which areas require human input, like deciding on treatments and solutions after looking at the prognosis.
A few months ago, on an Arizona biotech panel, he said, he learned that 70-80% of a physician’s time is spent on paperwork and getting a patient’s records together, instead of actually seeing the patient. AI will allow automatic transcription and summarizing of information, so physicians can spend more time interacting with and treating patients, Ebert said.
Transformations like this could also help ease the national crisis of a scarcity of primary care physicians, he said, because not as many doctors would be needed if each was spending more time with patients.
Overall AI use in health care
Ebert said the intersection of AI and health has been underway for some time, but the accelerating pace of adopting the technologies is starting to show more promise to drastically change the way health care is delivered.
He hopes that in five years, for example, there will be lightweight sensors connected to people’s phones that will analyze everything going on in their bodies. If and when these sensors detect an anomaly in the body, they’ll automatically inform the person’s doctor, and the doctor can immediately begin an informed conversation about treatments.
“This idea of being able to detect disease before you even feel the symptoms is what we’re starting to be able to do now. This has occurred, for instance, with respiratory syndromes and COVID, many other things where basically, we have detection now — that just from a single breath, you can detect someone has something from five to 14 days before they start showing symptoms,” Ebert said.
“And if you think about being able to detect the first instance of cancer cells that are not being responded to by T cells in a body, and being able to take proactive action at that point, you can make a huge difference.”
Another example he gave of using AI in health care would be during a biopsy or genetic makeup of a specific cancer. AI could be used to look at all potential variations and genetic mutations that might occur, and create therapies that will allow T cells to recognize more than 50% of those. In these cases, medical professionals could create a shot or medicine for patients that would allow them to be cured at stage four of cancer, because they could get the person’s immune system to start immediately responding, Ebert said.
Gurtner said the use of AI in health care is going to transform medicine because the amount of data that exists right now is incomprehensible to humans. While it might take thousands of people to look through medical data and analyze trends, AI can very quickly identify trends and make correlations of what might actually happen to patients, he said. The data processing power of AI will be very helpful, he said.
He also hopes it “lowers cost and democratizes medicine.”
“There’s lots of things that are relatively automatable, and if we can automate the automatable things, I think it has the promise of decreasing costs and increasing access, which is kind of the holy grail right now,” Gurtner said.
Currently, he said, “We’re (going) in the opposite direction. We’re going to get rid of Medicaid for some patients. We have a very inefficient system that many patients can’t access, and it’s very expensive.
"So, I think technology lets you imagine a future where you have a lower-cost system that’s available to everyone, that is more efficient and costs everyone less.”
Researchers are projecting that 1.3 billion people will have diabetes by 2050 worldwide, more than double the current number.
Reporter Prerana Sannappanavar covers higher education for the Arizona Daily Star and Tucson.com. Contact her at psannappa1@tucson.com or DM her on Twitter.
Prerana Sannappanavar
Higher Education Reporter